Virtual follow-up for first appointment after hip and knee arthroplasty surgery is acceptable during the COVID-19 pandemic but not for routine practice
By Tomos Richards and Khitish MohantyCardiff and Vale Orthopaedic Centre, University Hospital Llandough, Cardiff
Corresponding author email: [email protected]
Published 24 June 2020
Introduction
The COVID-19 global pandemic has caused massive disruption to routine scheduled care in the United Kingdom and worldwide. In our university health board, cessation of elective surgery occurred on 15th March along with all non-essential clinic appointments. This led to a cohort of patients having undergone arthroplasty in the six weeks prior to 15th March being unable to attend for their routine first post-operative visit with this ‘check up’ undertaken by telephone call instead. Whilst virtual follow-up methods are well established in stable arthroplasty patients, to our knowledge it has not been used for first post-operative visits in the past. With potential cost and convenience advantages to both the patient and the health service, we aimed to assess patients' satisfaction with this method of follow-up to guide future practice in the post pandemic era.
Materials and methods
Local approvals were sought and obtained for the study. All patients who underwent hip and knee primary or revision arthroplasty between 3rd February 2020 and 15th March 2020 had received a phone call from their operating surgeon or a nominated deputy (fellow or registrar) in the six weeks following surgery. In this call they were given the opportunity to raise any questions and were assessed in a non-structured way similar to a routine clinic visit. Patients were asked to self report on the condition or any problems with their wound through a dedicated telephone number. Where there was any significant concern raised by the patient a face-to-face appointment was made to see the operating surgeon in the urgent clinic. Patients were then sent a structured questionnaire via email which can be viewed in Appendix 1. A second email was sent to all patients who were yet to complete the survey after one week, followed by a phone call to improve the response rate. Responses were collated to analyse patient’s perceptions of the service.
Results
57 eligible patients were identified in this period and sent the questionnaire, of which 50 (88%) returned a completed form. The mean age of respondents was 67 with a range of 46 to 84. There were 19 (40%) males and 28 (60%) females with 62% having undergone knee replacements and 38% having undergone hip replacements. Patient’s aims and expectations from the appointment mainly centered around three themes:
- Reassurance about progress
- Visual check of the wound/joint
- Advice on maintaining recovery/therapy
63% of patients felt that their aims and expectations were met from the ‘virtual’ appointment. Six of 44 (14%) responses stated they had a concern regarding their wound at some time following the surgery and 26% sought advice regarding a concern following their operation. On a five point Likert scale 74% found this method quite or very convenient, 68% felt it was quite or very effective, and 62% were quite satisfied or very satisfied. These results are shown graphically in Figures 1-3.
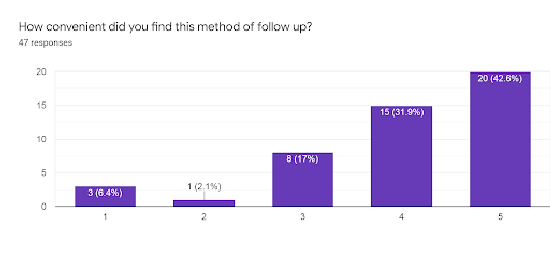
Figure 1: Displaying convenience from 1 - Not at all, to 5 - Very much so
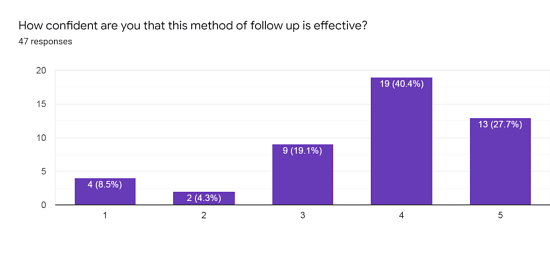
Figure 2: Displaying patients’ confidence from 1 - Not at all, to 5 - Very much so
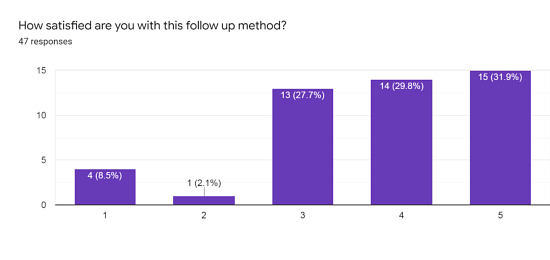
Figure 3: Displaying patients’ satisfaction from 1 - Not at all, to 5 - Very much so
There were no statistically significant differences in convenience, confidence or satisfaction ratings with age or sex or procedure undertaken. 66% of respondents felt that this method had saved them time and 39% felt it had saved them money. 59% of respondents felt this method was worse than a usual clinic appointment and only two patients (4%) felt it was better. 57% of patients felt they were missing out on something by not seeing their surgeon face-to-face. Overall 75% of patients preferred to have future appointments face-to-face, 11% would prefer telephone, 13% would prefer a video call and 2% would prefer a web-based questionnaire, (Figure 4).
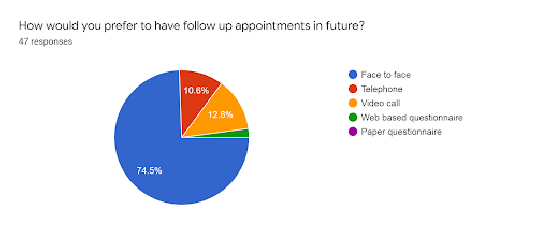
Figure 4: Displaying patients’ preference for future follow-up
The mean age of patients preferring face-to-face appointments (65.8) had a trend to be lower than that of those preferring other virtual methods (70.3), however this did not reach statistical significance with p= 0.072. Some key quotations from free text answers are shown in Figure 5.
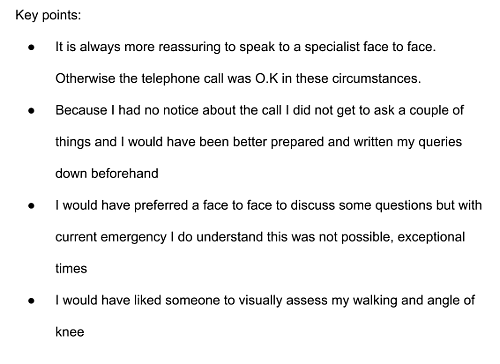
Figure 5: Showing key quotations from patients’ responses to white space questions
Discussion
Hip and knee arthroplasty numbers continue to grow with over 100,000 of each performed each year in 20161. This continues to put a significant burden on the healthcare system which is under ever increasing pressure to provide cost effective solutions. The British Orthopaedic Association have published guidance suggesting follow-up in person at six weeks post-operatively for hip and knee arthroplasty, followed by a ‘virtual appointment’ at one year2,3. These virtual appointments have been shown to have high patient satisfaction rates4 and safety5. Due to the introduction of social distancing and cancellation of non-essential services it was necessary to perform virtual follow-up at the six week stage for a cohort of patients in our unit. These were patients that underwent their elective arthroplasty surgery in the six weeks prior to the cessation of services on the 15th of March due to COVID-19. This gave us a unique insight into the feasibility and acceptance of a virtual clinic appointment for the first appointment after surgery at six weeks post-operative.
Three key themes for patients expectations for their six week appointment were illustrated in the survey. Reassurance regarding their progress and guidance regarding maintaining their recovery is accomplishable by telephone conversation although some communication through body language and gesturing may be lost. A visual inspection of the wound and joint is however impossible to achieve through a telephone consultation alone. We had to rely on patients’ description and their own concerns about the wound and where there was any doubt then a face-to-face appointment would have to be made. Another important aspect of an early appointment is to monitor rehabilitation and regaining of strength and mobility of the operated limb. It is not feasible to assess the muscle weakness, range of motion and strength of the joint virtually. Similarly leg length assessment and institution of remedial measures like shoe raise and physiotherapy would be very difficult by any virtual settings. A potential option to aid with some of this assessment would be the use of a video call which has become a widely used method of communication in the COVID-19 pandemic. This would be the preferred method of communication for 14% of respondents surveyed.
Despite this lack of a visual check up, satisfaction, confidence and convenience ratings were high amongst respondents. Many felt that they had saved time and some had saved money using this method. Certainly it is a cost and time saving method for the healthcare service itself. Despite these ratings many patients referenced the fact that they felt the service was acceptable because of the current pandemic and not in normal circumstances. This is reflected in the fact that 57% of patients felt they missed out on something by not seeing their surgeon face-to-face, and 75% of patients would prefer to have their further appointments face-to-face. The trend for more elderly patients to prefer virtual clinics may reflect the convenience of not having to travel, and the more low demand nature of this cohort.
As a lifelong procedure, direct feedback about the operation and perioperative issues by the treating surgical team is crucial and requires effective communication. Recognition and remediation of post-operative problems are vital as many are time critical. Also important is the feedback provided by their patients to aid development and progression of an individual surgeon’s and departmental practice. Face-to-face post-operative contact is therefore also vital to the arthroplasty surgeon as well as the patient.
There are some limitations to this study, the first being the response rate. Whilst a rate of 88% is excellent given the method of voluntary patient survey, there is a potential for bias, especially as questionnaires were completed electronically which may overemphasise the opinions of more technologically familiar individuals. Familiarity with internet skills is increasing and in 2018 only 10% of the UK population were classed as internet non-users according to the office of national statistics so we feel this method of distribution not to be unreasonable6.
Despite this we feel the study has shown that a virtual follow-up for six week post arthroplasty appointment is satisfactory when conditions do not allow patient attendance in person. We have learnt from patient insights into the service and there are a number of improvements we would make in future. Prior notice and a formal appointment time would allow patients to prepare thoughts and questions for the appointment. This would also allow dissemination of written advice which can guide future therapy and recovery, and answer many common questions in advance. The use of video call would allow a visual inspection of the joint and wound and give both the patient and surgeon more confidence in the recovery.
Certainly this method of follow-up will not replace face-to-face visits for routine six week post-operative appointments, but we hope it provides some insight into guiding how to manage such virtual appointments should the need arise again in this uncertain future and during the reinstatement of elective services.
References
- National Institute for Health and Clinical Excellence (2018). NICE guideline: Hip, knee and shoulder joint replacement draft scope for consultation. Available at: https://www.nice.org.uk/guidance/GID-NG10084/documents/draft-scope.
- British Orthopaedic Association (2017). Pain arising from the hip in adults – Commissioning guide. Available at: https://www.boa.ac.uk/resources/pain-arising-from-the-hip-guide-final-pdf.html.
- British Orthopaedic Association (2017). Painful osteoarthritis of the knee. Available at: https://www.boa.ac.uk/resources/painful-oa-knee-guide-final--pdf.html.
- Ferdinandus S, Smith L, Pandit H, Stone H. Setting up an arthroplasty care practitioner-led virtual clinic for follow-up of orthopaedic patients. British Journal of Nursing. 2019;28(20):1326-30.
- Fisher R, Hamilton V, Reader S, Khatun F, Porteous M. Virtual arthroplasty follow-up: five-year data from a district general hospital. Annals RCS. 2020;102(3):220-4.
- Office for National Statistics (2019). Exploring the UK’s digital divide. Available at: https://www.ons.gov.uk/peoplepopulationandcommunity/householdcharacteristics/homeinternetandsocialmediausage/articles/exploringtheuksdigitaldivide/2019-03-04.