ORTHO-ALERT – Setting up a departmental bulletin of shared learning from surgical mistakes and masterpieces
By Robyn Brown
Orthopaedic ST5, Severn Deanery
Mistakes, near-misses, and masterpiece moments happen in orthopaedics. Every time, a learning opportunity arises for the individuals involved and the wider orthopaedic community. Sharing learning not only to promote a positive culture, but also to lessen the likelihood of incidents being repeated by another unsuspecting surgeon.
Although the actions of seniors set a precedence for juniors to follow, organisational factors undoubtedly play a huge role in encouraging or discouraging shared learning. The aviation industry has recognised this and employ a system of voluntarily submitted incident reports, immunising reporters from blame, with dissemination of the learning points to the whole aviation community to lessen the likelihood of repeat events. This is known as the Aviation Voluntary Safety Reporting System (ASRS).
This effective idea is incredibly translatable to the NHS. Inspired by the aviation industry, a similar no-blame learning initiative was piloted at a single orthopaedic department, has now been rolled out in several trusts, and can be easily implemented within trusts: ORTHO-ALERT.
What is ORTHO-ALERT?
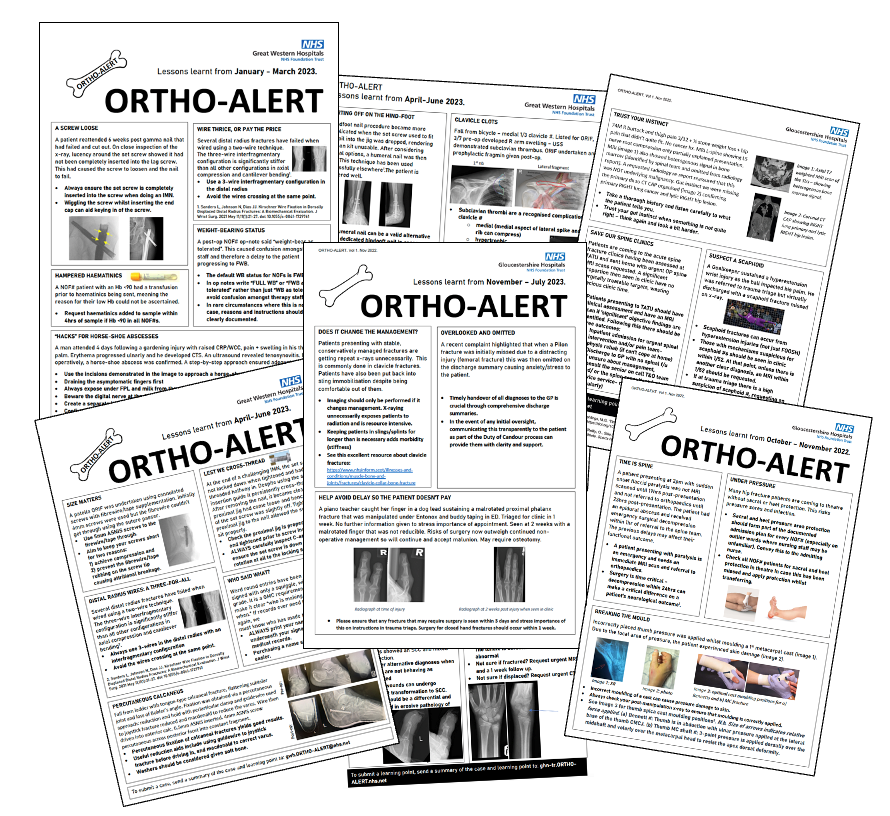
ORTHO-ALERT is a quarterly bulletin of shared learning from intra-departmental surgical mistakes and masterpieces. It allows any department member to submit key technical tips, practical pointers, or even administrative advice to a dedicated email address easily and without copious form-filling administration. Case submissions are received by the nominated six-monthly middle grade editor, anonymised and key learning points confirmed. Anonymised cases are then compiled into a bulletin format and disseminated periodically as a PDF email and a printed bulletin displayed above theatre scrub sinks. This gives the whole orthopaedic department equal access and opportunities to both submit learning points and learn from others. Those who repeatedly can’t make Morbidity and Mortality (M&M) meetings can have access to its learning. Those who have been frustrated at repeated mishaps have a pro-active way to distribute tips. Those exposed to feedback after an exhausting on-call can now approach it constructively in their chosen time.
ORTHO-ALERT has had unanimously positive feedback from both those submitting and reading. It is creating a psychologically safe, positive learning culture for surgeons to share experiences.
How do I set up ORTHO-ALERT in my department?
- Request the toolkit.
Please email [email protected] for a copy of the ORTHO-ALERT toolkit which includes a how-to guide, advertising poster template, bulletin template, and certificate template.
- Assign a consultant lead.
This naturally suits the local governance lead but can be any interested consultant, their role being to encourage departmental buy-in, oversee and proof-read the bulletin prior to its distribution.
- Set up a dedicated email address.
Liaise with your IT support to create a simple email address that people will be able to find easily after typing a few letters (e.g. [email protected]). Make sure both the consultant lead and editors can obtain access to it with ease.
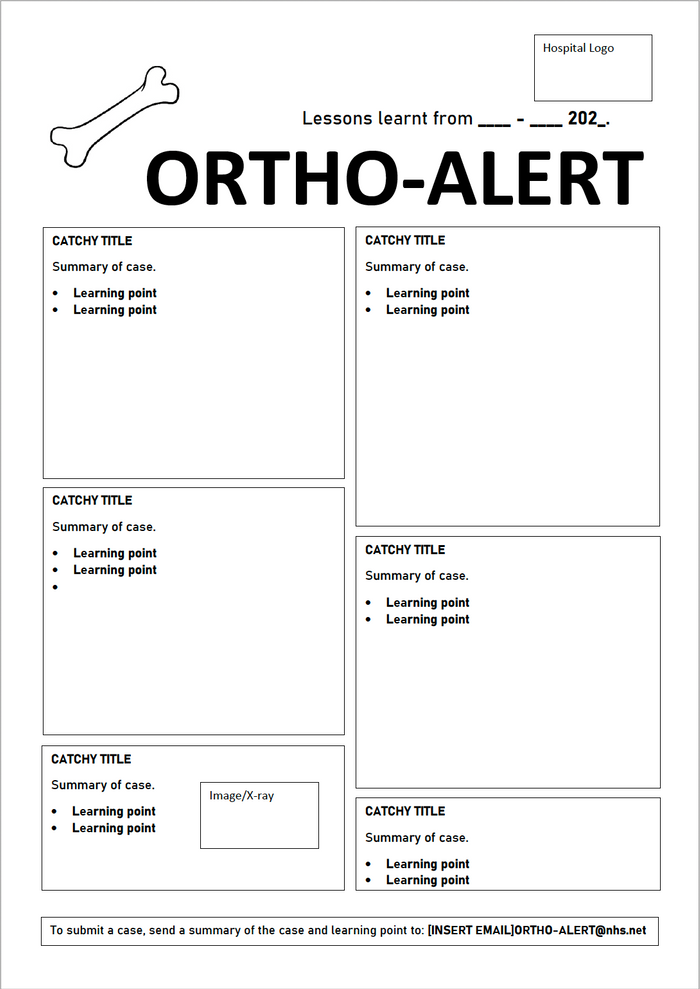
- Use the bulletin template.
Bulletins are designed with ease on Microsoft Powerpoint and saved as PDFs. Utilising the bulletin template below can make designing and formatting very easy and standardised.
- Assign rotating editors.
This role typically suits a registrar. It nicely demonstrates involvement in governance activity needed for CV portfolios and completion of training (CCT) requirements. It involves compiling and distributing a bulletin from a template every 3-4 months (typically taking several hours). This role can be passed on every six months to allow opportunities for multiple registrars and maintain manageable workloads. Every participating registrar can be supplied with a portfolio certificate.
- Promote submissions within the department.
Introducing the concept of ORTHO-ALERT at local trauma meetings, audit meetings and via email (from the submission email address) can be supplemented with laminated posters in theatres, clinic rooms, and coffee rooms displaying the submission email address. Reminding colleagues to submit when they are discussing appropriate cases in trauma meetings, coffee rooms and after cases also helps to get the ball rolling.
- Compile bulletin
Every three months, the editor will review the inbox, summarise the submissions into the bulletin template and insert any useful images accompanying cases. The consultant lead should then check the content.
- Distribute
The bulletin should be distributed via email to the department. It should also be printed, laminated, and placed above theatre scrub sinks or in coffee rooms where possible.
How do I sustain ORTHO-ALERT in my department?
- Incorporate 'anything for ORTHO-ALERT?' into the WHO sign-out (and ask someone to do the submission!)
- Assign someone responsible for printing, laminating, and placing printed ORTHO-ALERTs in theatres, coffee rooms, and doctor’s offices when they are emailed out.
- Send departmental reminders via email before the submission deadline.
- Assign registrars through a systematic approach (i.e. always the lead consultant’s registrar or the chief registrar).
- Agree distribution dates at the start of each registrar tenure.
- If submissions are lacking at times, supplement them with 'Datixes' (trust electronic incident reporting systems) or M&M cases.
What next?
If you would like to set up ORTHO-ALERT within your trust or in your deanery, please don’t hesitate to contact me for advice or help to get the ball rolling at [email protected].
Although local bulletins are vitally important to ensure that learning from bulletins remains highly relevant to readers, and in a psychologically safe environment, ORTHO-ALERT should pave the way for a further national-level submission and bulletin distribution system of key learning point. Any surgeons should be able to submit a case without fear of investigation and the learning points distributed via national email networks on a regular basis for surgeons to all learn from each other.
The author would like to thank Will Mason, Consultant Orthopaedic Surgeon, Gloucestershire NHS Foundation Trust and Andrew Tasker, Consultant Orthopaedic Surgeon, Great Western Hospital for their support with this project.