From Medical School to T&O Consultant - the gender specific pipeline is leaking…
by Emily Clough
3rd year Medical Student at the University of Manchester
|
This essay was runner-up in the 2021 BOA Medical Student Essay Prize As a medical student, what would encourage you to consider a career in T&O and what are the perceived barriers to such a career? |
‘If you can see it, you can be it ...’
…but what if you can’t see it?
Attractions of Trauma and Orthopaedics (T&O) as a career: an incisive choice
The BOA website advertises Trauma and Orthopaedics (T&O) as an ‘extremely rewarding career’1, a unique specialty facilitating the ability to transform a patient’s life - to relieve pain, heal trauma, reverse disability - all while stimulating the creative and practical dexterities of the surgeon. As a medical student, the career is incredibly attractive. Who would not want to transform a patient’s life with a joint replacement, or restore a smashed limb back to function? T&O surgery appears highly efficacious, with the total hip replacement (THR), having been described as the ‘operation of the century’2. It is one of the most powerful of any elective surgical procedure, with the number of quality-adjusted life years (QALY) gained reported as 6.5 and a cost/QALY of £1,3723. The National Institute for Health and Care Excellence (NICE) has a current cost-effectiveness threshold of £20,000/QALY4, and many orthopaedic surgical procedures not only fall well below this threshold Incremental Cost-Effectiveness Ratio (ICER), but perform competitively against surgery from other specialities (see Table 1). So, with T&O having so many positive features, it should not need much encouragement to be considered as a career.
|
Table 1: Comparing T&O £ cost/QALY scores to those from other surgical specialties |
|
|
Surgical Procedure |
ICER (£ cost/QALY) |
|
THR3 |
1,372 |
|
TKR3 |
2,101 |
|
TSR4 |
2,439 |
|
Laparoscopic cholecystectomy5 |
15,742 |
|
Hernia Repair5 |
10,054 |
|
Varicose vein treatment6 |
26,107 |
|
THR total hip replacement, TKR total knee replacement, TSR total shoulder replacement ICER incremental cost-effectiveness ratio |
|
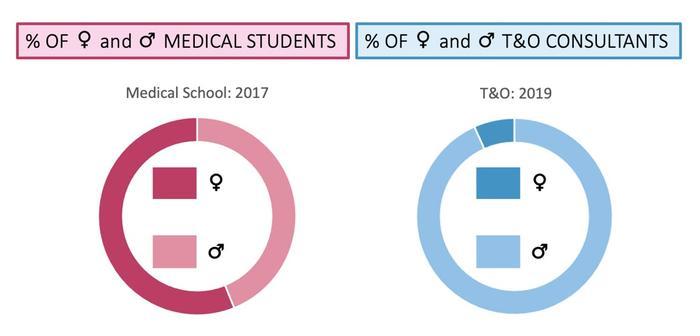
So then, what are my barriers? Unfortunately, there is significant disparity in the ratio of female to male Consultants within the profession. T&O has the lowest female Consultant ratio of all the surgical specialties (4.6% in 2011)7. By 2019, the number of female Consultants within T&O had risen only slightly to 6.7%8. This is despite the fact that since 1996, there have been more female entrants to medical school than male9 and by 2018, 57.1% of medical school entrants were female10. This lack of diversity is not seen as acutely in other specialties. As of 2019, the UK National Health Service (NHS) employed 1,242,507 staff11. 119, 597 of these were doctors, of which 53,976 were female (45.1%). In total, across all specialties, there were 51,043 consultants, of which 18,802 (36.8%) were female8. However, there are now more female than male consultants in Clinical Genetics (77.7%), Palliative Medicine (76.6%), Dermatology (63.2%), Obstetrics and Gynaecology (57%), Paediatrics (56.2%) and Medical Oncology (53.7%)8. Diversity is essential for creating strong organisations, improving performance, attracting the best talent, strengthening decision making and increasing innovation12. Understanding the current state of diversity within the field of T&O, where the pipeline from Medical School intake is leaking, and why so few females are specialising in T&O, is imperative to successfully attract, train, and retain the next generation of T&O surgeons.
Dissecting the Problems…
There are several reasons proposed as barriers for aspiring females entering a career in T&O as highlighted in Table 2. For students considering commitment to the specialty, lack of exposure to T&O in the medical school curriculum means trainees rely on the experience of others, and the unconscious bias and stereotypes that exist within general culture to form opinions. With this lack of personal exposure, students are left to draw conclusions from the evidence presented. Whilst this can limit both male and female recruitment, it is arguably magnified for females.
|
Table 2: Barriers to T&O for women found in the Medical Literature |
|
|
Perceived Barrier |
Evidence validating Perceived Barrier for Women |
|
Lack of female role models, supervisors, trainers and mentors in the field makes it hard for students to visualise, and ultimately to realise. |
Orthopaedic training programmes with a greater representation by female faculty have a higher proportion of female trainees12. However, males who are good advocates and mentors for females are equally positive, and cross gender mentoring remains vital to achieve equity. |
|
A perceived unconscious bias of a ‘hidden curriculum’ and stereotype. |
Surveys have identified a wide-spread perception that orthopaedic surgery is an ‘old boys’ club’ of heavily built, macho, rugby playing males, and that you cannot be a mother and an orthopaedic surgeon, as the work-life balance is too difficult13. A study reported 24% of medical students would consider a career in orthopaedic surgery, but 62% of females were deterred following exposure to negative attitudes towards female surgeons14. |
|
An existing perception of a lack of flexibility in the training program, lack of time for family, friends and parenting, and surgical work hours acting as deterrence to pursuing a surgical career. |
Female trainees more likely to perceive this as restrictive compared to their male peers15,16. Countries advertising the most generous parental leave and progressive social policies - Sweden and Estonia – have the highest rate of female participation internationally (16.8% and 26.4% respectively)12. |
|
The practical demands of operating whilst pregnant, especially in the third trimester, of wearing lead aprons and standing for long periods, cause anxiety, and are a challenge for those considering future family plans. |
Data reporting the specific effects of pregnancy and breastfeeding for the female surgeon are a concern and challenge. Data from the USA reports the risk of complications in pregnancy are higher for female orthopaedic surgeons (31.2%) compared to the general population (14.5%) (17). |
Stitching together solutions: Inclusive encouragement
Having identified the barriers and challenges that females face in choosing and pursuing a career in T&O, strategies have been, and can continue to be formulated, to encourage young females into the specialty.
In 2019, the BOA developed a strategic policy document, with a three year aim to change, identifying key areas, including increasing diversity within the BOA leadership, increasing diversity at Congress and events, increasing T&O awareness as a career option and providing support to maintain an interest throughout the T&O career. Schemes such as the Less Than Full Time (LTFT) training, whereby childcare is a prioritized reason for acceptance of LTFT18, and the Supported Return To Training (SuppoRTT) program19 have been created to challenge the perceptions held by many students deterred from T&O.
Highlighting gender diversity in T&O from an early point in a student’s medical career is beneficial for change. The ‘Future Women in Orthopaedic Surgery’ conference, held in 2019 is testament to this, as a questionnaire following the Conference reported 93% of participants felt they’d gained knowledge regarding breaking down personal barriers to specialising in T&O, and 95% felt the education they had received stimulated aspiration to pursuing a T&O career9.
Between 2014 and 2019, only 2 of the 29 named lectures (7%)20 at the BOA congress, an event epitomising the British Orthopaedic community, were by female speakers; one a motivational speaker and the other, the former President of RCS England. Having an outreach session for aspiring female medical students, displaying gender diverse representation, could act to challenge any established perception of T&O being a male governed culture. Previous BOA medical student competitions have encouraged exploration of the use of Social Media platforms. Utilising the fresh and contemporary ideas of my predecessors, the promotion of gender inclusive material could be fruitful (see Table 3).
|
Table 3: Possible promotion suggestions using inspiration from ideas pitched in the 2020 Medical Student Essay Prize, ‘Mind the gap between the (orthopaedic) train(ee) and the (social media) platform’ |
|||
|
Social Media Platform |
BOA account |
Suggested uses by previous Competition Winner |
Specific to Gender Diverse Engagement |
|
|
British Orthopaedic Association |
Events Live stream webinars |
|
|
|
@britorthopaedic
|
Tips and pathways for a career in Orthopaedics |
|
|
Website |
www.boa.ac.uk |
|
Create a medical student tab: could be used to summarise the existing information on training pathway, schemes such as LTFT, and link events or contacts for outreach officers |
Conclusion
Earlier promotion of the concept that females can be Orthopaedic Surgeons is the most critical step in breaking the perceived barriers to a career in T&O for female medical students. Some strategies have already been established to navigate the barriers discussed in this article, but more emphasis on the promotion of these strategies is needed, as this has proven to be successful in inspiring and motivating young female medical students as demonstrated by the ‘Future Women in Orthopaedic Surgery’ conference. There, Miss Swee Chai Ang, the first Female Orthopaedic surgeon appointed at the Royal London Hospital (1994), was asked, “How can females become an orthopaedic surgeon?” She replied, “By being human, being a doctor, being a surgeon and being themself”9 - a message that should be more clearly heard by female medical students - like myself - filled with enthusiasm, optimism and aspiring to a career in T&O.
References
- British Orthopaedic Association. Careers. [cited 21 April 2021]. Available from: www.boa.ac.uk/careers-in-t-o.html.
- Learmonth ID, Young C, Rorabeck C. The operation of the century: total hip replacement. Lancet. 2007;27:1508-19.
- Jenkins PJ, Clement ND, Hamilton DF, Gaston P, Patton JT, Howie CR. Predicting the cost-effectiveness of total hip and knee replacement: a health economic analysis. Bone Joint J. 2013:95B:115-21.
- Nicholson JA, Jones R, MacDonald DJ, Brown I, McBirnie J. Cost-effectiveness of the reverse total shoulder arthroplasty. Does indication affect outcome? Shoulder Elbow. 2021:13:90-7.
- Chen TC, Wanniarachige D, Murphy S, Lockhart K, O’Mahony J. Surveying the cost-effectiveness of the 20 procedures with the largest public health services waiting list in Ireland: implications for Ireland’s cost-effectiveness threshold. Value in Health. 2018;21:897-904.
- Brittenden J, Cotton SC, Elders A et al. Clinical effectiveness and cost-effectiveness of foam sclerotherapy, endovenous laser ablation and surgery for varicose veins. Health Technol Assess. 2015:19:1-342.
- Royal College of Surgeons of England (2011). Surgical Workforce 2011. A report from the Royal College of Surgeons of England in collaboration with the surgical specialty association. Available from: www.rcseng.ac.uk/library-and-publications/rcs-publications/docs/surgical-workforce-report-2011.
- NHS Digital (2019). HCHS doctors by specialty group, specialty, grade and gender, Sept 2009 to March 2019 AH2736. Available from: https://digital.nhs.uk/data-and-information/find-data-and-publications/supplementary-information/2019-supplementary-information-files/hchs-doctors-by-specialty-grade-and-gender-sept-2009-to-march-2019-ah2736.
- Nguyen ATV, Al-Shawk M, McNally S, Hing CB. Should women do orthopaedics? Journal of Trauma & Orthopaedics. 2020;8(1):20-1.
- General Medical Council (2020). The state of medical education and practice in the UK. Available from: www.gmc-uk.org/about/what-we-do-and-why/data-and-research/the-state-of-medical-education-and-practice-in-the-uk.
- NHS Digital (2018). Analysis of the representation of women across the hospital and community health service workforce. Available from: https://digital.nhs.uk/data-and-information/find-data-and-publications/supplementary-information/2018-supplementary-information-files/analysis-of-the-representation-of-women-across-the-hospital-and-community-health-services-workforce.
- Green JA, Chye VPC, Hiemstra LA, et al. Diversity: Women in orthopaedic surgery - a perspective from the International Orthopaedic Diversity Alliance. Journal of Trauma & Orthopaedics. 2020;8(1): 44-51.
- Miller EK, LaPorte DM. Barriers to Women Entering the Field of Orthopaedic Surgery. Orthopedics. 2015; 38(9):530-3.
- Bucknall B, Pynsent PB. Sex and the orthopaedic surgeon: a survey of patient, medical student and male orthopaedic surgeon attitudes towards female orthopaedic surgeons. Surgeon. 2009;7(2):89-95.
- The Royal Australasian College of Surgeons (2020). Breaking Barriers Developing Drivers for Female Surgeons Survey. Available from: www.surgeons.org/-/media/Project/RACS/surgeons-org/files/operating-with-respectcomplaints/Break-barriers-report_2020.pdf.
- Giantini Larsen AM, Pories S, Parangi S Roberston FC. Barriers to Pursuing a Career in Surgery: an institutional survey of Harvard medical students. Ann Surg. 2021 Jun 1;273(6):1120-6.
- Hamilton AR, Tyson MD, Braga JA, Lerner LB. Childbearing and pregnancy characteristics of female orthopedic surgeons. J Bone Joint Surg Am. 2012;94(11):e77.
- Nguyen ATV, Hing CB, Trompeter A. Less than full time training: being a parent and an orthopaedic trainee. Journal of Trauma & Orthopaedics. 2020;8(1):35.
- Campbell T. Supporting orthopaedic trainees returning to training after taking time out of programme. Journal of Trauma & Orthopaedics. 2020;8(1):40-42.
- Krahelski O, Gallivan S, Hing CB. How well are women represented at orthopaedic conferences? The Bulletin – Royal College Surgeons of England. 2020;206:382-6.